On Wednesday, I head to the hospital. I will be operated on by Dr Crary—an orthopedic surgeon specializing in feet. Here is what is going on:
My left foot (with apologies to Christy Brown and Daniel Day Lewis): Left peroneal longus to brevis transfer. possible hamstring allograft, lateralizing calconeal osteotomy, dorisflexing midfoot osreotomy gatronocnemic recession. Left cavovaruss foot, peroneal tendinitis, gastrocenmis equinus.
I will be bed-ridden for 14 days, beginning Thursday, August 9, 2018,. This will be to keep my foot elevated above my heart. This will reduce the swelling and minimize the chance for blot clots, etc. I will be allowed to get up 3X a day for meals and a tiny bit of exercise. I will do leg lifts, weights lifts for my arms, etc to try an reduce the inevitable atrophy. After this initial 2 weeks, I will have 4 weeks with a cast then 4 weeks in a boot. After that it will take about 40 weeks (total of about a year) for me to get back to “normal.” This seems like too much time—but it is what the “experts” are saying. All of this is a result of a congenital condition that caused me to “super pronate”–a big word meaning that on my left foot I walked on the outside edge. Time caught up with me and the two outside tendons, which were taking the load, are worn to the point of breaking. I do have a very positive attitude and hope to be able to post stories about the process.The surgeon will repair and strengthen these tendons and make some strategic “cuts” of my ankle and the bone to my left toe to “realign and drop my high arch; enabling my weight to be properly distributed.”
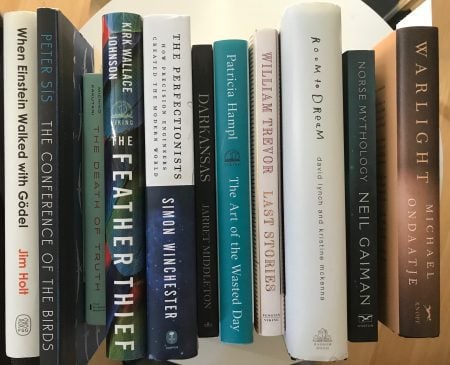 I have assembled my reading “pile” for the 12 weeks. I am already half way through the Room to Dream biography/autobiography about and by David Lynch. I suspect that I will plow through these books too quickly—but I also will have at my ready my sketch books. I want to plan my next 3 paintings.
I have assembled my reading “pile” for the 12 weeks. I am already half way through the Room to Dream biography/autobiography about and by David Lynch. I suspect that I will plow through these books too quickly—but I also will have at my ready my sketch books. I want to plan my next 3 paintings.
I have an idea for 3 “portal” paintings that will be based on people coming from a brightly lit corridor into a room that is dark. This will create a back-lit image. It is evocative of what we are facing in today’s heated and scary political world. We have left the enlightenment of the Obama presidency and are all entering a dark place occupied by many nefarious folks who are hell-bent on destroying our democracy.
We shall see how this plays out. In the meantime, stay tuned for the progress. I am especially interested to “self observe” this whole phenomenon since I am not one who likes sit still.
Time worn sayings are most appropriate for your condition:
“Do what the Doctor tells you to do”,
I’m thinking that in your case this will go without saying but wanted to mention it again.
Thanks John–the main issue is pain medicine. I do not like any pain medicine–but all advise tells me that I must manage pain for the first 72-96 hours to ensure long-term health benefits and avoid chronic pain latter on. Hope you are well
I am empathic with your plight, Jeff. I suspect the hardest part for you will be the recovery time which will greatly limit your activity. I’ve got to be making a decision soon about my arthritic ankle. I believe I will have my surgery done after Christmas with recovery during the winter months.
Anyway, all the best my friend. I look forward to hearing about your progress through recovery. It will give me some insight into what is in store for me. Take care! Bill Marks
Bill-it was a tough decision–but after seeing my MRI there was no question!
Thank you for informing us who care about you. Let us accompany you on this rocky road you had not contemplated taking, and we shall assist in every possible way, giving you a hand or emotional support as needed.
What courage and valor you exhibit. Know that you are much loved by many, and all will rally around you when the going gets tough.
From the bottom of my heart to the bottom of your foot!
As a former distance runner and pronator who long suffered through foot and ankle pain, I’m confused by your description of super-pronation as walking on the outside edge of the foot. Under-pronation is the term I’ve always heard applied to that condition.
Anyway, I hope you do well, and be sure to stick with the therapy. The muscle atrophy from inaction can be astonishing.
Hi Charlie–I am not a very “medical person” –what I am writing is what my doctor said. I will ask Dr Crary on Wednesday. But based on the following, I have “supination’! The following comes from http://stretchcoach.com/articles/pronation-supination/
What is Pronation?
Pronation refers to the inward roll of the foot during normal motion and occurs as the outer edge of the heel strikes the ground and the foot rolls inward and flattens out. A moderate amount of pronation is required for the foot to function properly, however damage and injury can occur during excessive pronation. When excessive pronation does occur the foot arch flattens out and stretches the muscles, tendons and ligaments underneath the foot.
The picture on the right (used from the steenwyk.com web site) shows a view of the right foot as if looking at it from behind. As you can see in the picture the ankle is over-pronating or rolling inwardly.
Pronation or rolling inwardly
What is Supination?
Supination (or under-pronation) is the opposite of pronation and refers to the outward roll of the foot during normal motion. A natural amount of supination occurs during the push-off phase of the running gait as the heel lifts off the ground and the forefoot and toes are used to propel the body forward. However, excessive supination (outward rolling) places a large strain on the muscles and tendons that stabilize the ankle, and can lead to the ankle rolling completely over, resulting in an ankle sprain or total ligament rupture.
This time, in the second picture to the right (used from the steenwyk.com web site), the foot is over-supinating or rolling outwardly.